 Clinical Trials Vendor Medidata to Go Public
Clinical Trials Vendor Medidata to Go Public
This is a new twist by today’s economy with little or very few companies taking the plunge to go public. I just briefly looked at the we...


Four Preview Videos in the Footer
Clinical Trials Vendor Medidata to Go Public
This is a new twist by today’s economy with little or very few companies taking the plunge to go public. I just briefly looked at the we...
 Cook Medical Unveils MicroWires to support Leg Therapy - Peripheral Arterial Disease
Cook Medical Unveils MicroWires to support Leg Therapy - Peripheral Arterial Disease
Cook Medical has quite an extensive product line with catheters, especially those impregnated with antibiotics to help keep infection rate...
 Bill Gates and Oliver Sacks to speak at Technology, Entertainment, Design conference (aka TED)
Bill Gates and Oliver Sacks to speak at Technology, Entertainment, Design conference (aka TED)
Additional information can be found on the website for the sold out event. If you haven’t taken in the website, I highly recommend taking ...
 2 hospital executives indicted in alleged fraud scheme in Los Angeles
2 hospital executives indicted in alleged fraud scheme in Los Angeles
This is a follow up on the City of Angels Medical Center where the homeless were being given medical care they did not need in exchange for...
 What happens when a drug is facing patent loss – create a new drug that with time or delayed release properties
What happens when a drug is facing patent loss – create a new drug that with time or delayed release properties
Now there’s one more alternative medication for GERD, soon to be released from Takeda as Prevacid nears patent expiration. As the article ...
 Complete Genomics to Release Its DNA Sequencing Data Next Week
Complete Genomics to Release Its DNA Sequencing Data Next Week
This is perhaps one of the most awaited announcements with Complete Genomics, who is basically slated to use their technology to “wholesale”...
Drinkers being penalized by insurance firms - UK
One more item being scrutinized for healthcare insurance from the UK, and the article states the insurance company can check with the appli...
Doctor's offices using online business intelligence software to determine the amount to collect
It is confusing today not knowing what is covered and how much, thus many doctors offices are checking online to find out what they can to ...
 Rediscovering the 'Joy' of it all - “Joy of Sex” has been Updated
Rediscovering the 'Joy' of it all - “Joy of Sex” has been Updated
We are definitely living in a different world than where we were in 1972. The new release has been all over the news of late and states th...
 Obsessed with having babies? Update on the Octuplets Story
Obsessed with having babies? Update on the Octuplets Story
With 6 children and adding 8 more, how will she be able to afford to raise all of them is the big question. One physician said anyone who ...
 The Medical Quack is now a Fan of Lance Armstrong and LiveStrong
The Medical Quack is now a Fan of Lance Armstrong and LiveStrong
LiveStrong is the site of Lance Armstrong with his world wide mission to bring an awareness to cancer through out the world. He now has a ...
 George Church Talks about DNA Genomic Mapping in Plain Terms
George Church Talks about DNA Genomic Mapping in Plain Terms
First of all if you are not familiar with what this is all about, use the link below to watch a video that will help you comprehend what is...
 Most Hospital Patients Unable to Identify Their Physicians - Survey
Most Hospital Patients Unable to Identify Their Physicians - Survey
With many surgeons and nurses working from registries today, this might have something to do with the study. Under the related reading you...
Mother of octuplets has six other children
All one can say is that this is one huge family, and a bit costly for 7 weeks of hospital care prior to delivery too. Let’s see 8 plus 6 m...
 Bird Abatement - Business Intelligence and Data Logging with a Tablet PC
Bird Abatement - Business Intelligence and Data Logging with a Tablet PC
Since I like and totally make use of Tablet PCs, this is one that I could not pass up. I love the name of the program “Scarecrow”, it fits...
 Where are the Emergency Rooms in California - How Many hospitals have closed in the last 10 Years
Where are the Emergency Rooms in California - How Many hospitals have closed in the last 10 Years
The Los Angeles Times has put together a site whereby you can look up and see what services are available and where. Use the link below to g...
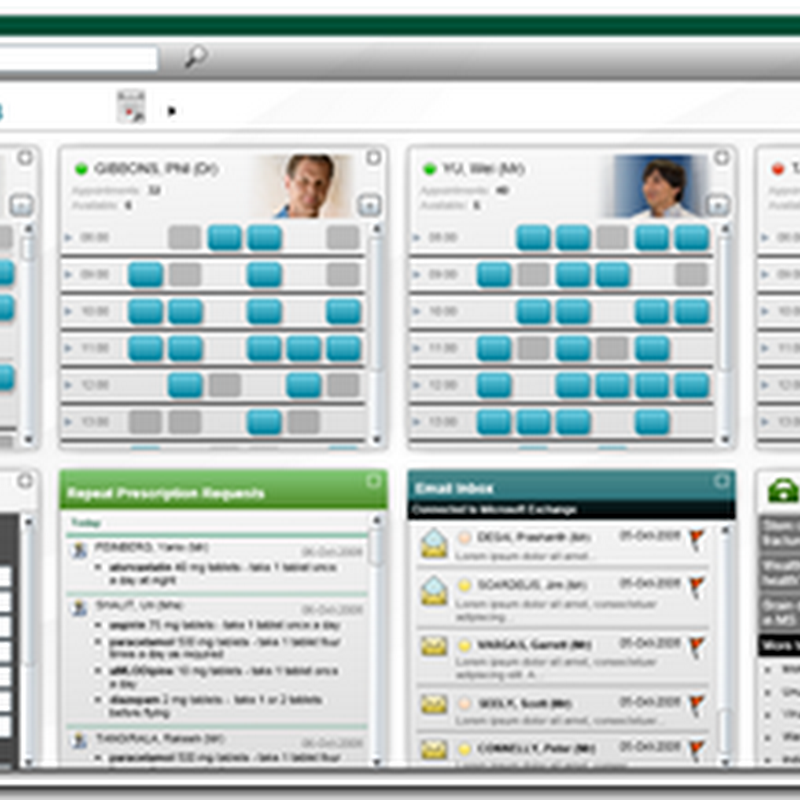
 Wisconsin Health Information Exchange RHIO connected with Amalga from Microsoft
Wisconsin Health Information Exchange RHIO connected with Amalga from Microsoft
Microsoft Amalga has been chosen to the software used to connect the network of hospitals. Each hospital was an “island” and had their own...