 This is pretty good and I felt compelled to include this as she’s the one before the programmers, in other words, Quants build models and programmers design and build it. In both videos you will find a lot of answers as she’s good and if you read here then you have probably heard a lot of this from a programming side. She’s the first step ahead and created the model that programmers use to write software. She has had a very interesting background and she digs in to big data and that subject I think be renamed, the “data scientist”…same thoughts where in the world do you find these people. You can find her blog here, MathBabe, like the name.
This is pretty good and I felt compelled to include this as she’s the one before the programmers, in other words, Quants build models and programmers design and build it. In both videos you will find a lot of answers as she’s good and if you read here then you have probably heard a lot of this from a programming side. She’s the first step ahead and created the model that programmers use to write software. She has had a very interesting background and she digs in to big data and that subject I think be renamed, the “data scientist”…same thoughts where in the world do you find these people. You can find her blog here, MathBabe, like the name. “Data Scientists”– An Oxymoron? Is Finding the Value in Data Bases Queried Together in the Business World To Make Money Actually Science?
She gives her background about being a young nerd and she has been a professor and later was hired by a Wall Street Hedge Fund as a Quant. She worked with Larry Summers who ended up going to work for the Obama Administration. Her idea at the time was to “fix” the system. Nobody including the SEC wanted to hire her and she says the same thing I have said many times, get the attorneys out and get the computer scientists folks in there. She said nobody cared with the models and some of the CDO models were completely broken and gave random numbers. Clients were never given fair warnings she said and she gave up and left and applied again to the Feds and and she signed forms to where she could not give away the private information on the models but she could talk about “techniques” of models and that’s what she does on her blog. Her idea is to help people, not exploit them. She says portfolios are “dummied” down into single numbers so those that think they understand can understand but they don’t really understand:) My thoughts from a short while back on risk.
Hiding, Falsifying, And Accelerating Risk Has Become the Achilles Heel of the US Economy As the “Real” World” Clashes With the Values Created From a World of “Fictional Values” Of Formulas and Math
Models are used increase obscurity and are not explained and are abused. I made my comments on models used out of “context”.  Avoid doing harm she states. She still models and knows the benefits when done correctly. Nerds are never in charge. I just talked with someone the other day where a study was done and the data was not supplied to substantiate the abstract and without the data, the recipient determined there were over 500 million available models, data counts and you just can’t take to the bank a report or study you see in the news without offering someone the opportunity to confirm the data origins, etc.
Avoid doing harm she states. She still models and knows the benefits when done correctly. Nerds are never in charge. I just talked with someone the other day where a study was done and the data was not supplied to substantiate the abstract and without the data, the recipient determined there were over 500 million available models, data counts and you just can’t take to the bank a report or study you see in the news without offering someone the opportunity to confirm the data origins, etc.
Big Data/Analytics If Used Out of Context and Without True Values Stand To Be A Huge Discriminatory Practice Against Consumers–More Honest Data Scientists Needed to Formulate Accuracy/Value To Keep Algo Duping For Profit Out of the Game
A little later on she talks about how models get used “that was a r eally useful model to make a lot of money”…you’ve had heard something like that here before:) People are trained to think of mathematics as a game you have to “win”, the culture in finance. No Quants are ever expected to answer or account for the consequences on the effects of normal people. Modeling has gone crazy and it has and it will.
eally useful model to make a lot of money”…you’ve had heard something like that here before:) People are trained to think of mathematics as a game you have to “win”, the culture in finance. No Quants are ever expected to answer or account for the consequences on the effects of normal people. Modeling has gone crazy and it has and it will.
You can speed up to around 18 minutes where the healthcare portion comes in. Think about 15 years from now she says, the information on the web about you never goes away. De-Identified data, she says the same thing I said a few years ago, people are good at matching up De-Identified data, heck I did it years ago and not for the purpose of selling data or anything of the sort, it was some algorithms that I wrote for integrating software and to check and balance myself I created sample data that would rematch in the system for billing and an automated super bill system.
Old hat been around a long time and a couple years ago the OMG stuff on the web about this being possible, that’s just when the  public woke up. It’s not that we are really that smart it’s just that we have “been there done that” way before a consumer even hears the concept, why we are geeks:) What is great about her videos is that she does for modeling about the same as I do for programming and there’s nothing like hands on as everyone else just reads other stuff and repeats it. She addresses both sides of healthcare data and says the clinical side is great and of course I agree, but then we have the health insurers who use segmentation in the opposite direction.
public woke up. It’s not that we are really that smart it’s just that we have “been there done that” way before a consumer even hears the concept, why we are geeks:) What is great about her videos is that she does for modeling about the same as I do for programming and there’s nothing like hands on as everyone else just reads other stuff and repeats it. She addresses both sides of healthcare data and says the clinical side is great and of course I agree, but then we have the health insurers who use segmentation in the opposite direction.
She did some other jobs and a lot with credit risks. Listen to her job offer about modeling in Hollywood and she’s see right through it with crazy modeling and how it keeps inequality alive. If you want to hear her points on healthcare move forward to around 16 minutes. Here’s a second video to where she talks at the Hadoop Strata Conference. She says you can’t just rebrand people from the inside and turn them into data scientists.
http://www.youtube.com/watch?v=3up4PezpthU
Here’s the series on the Attack of the Killer Algorithms that go right in line with what Cathy says and watch the videos and they are also on the left hand side of this blog on every page. If you want a look into reality on how math and formulas rule the world, spend the time and get a tiny bit of education to understand how this works quietly behind the scenes and how the algorithms shift and take your money, a few SQL “strings” at a time. BD
 drug is pretty hefty with warnings as well and is to be used after other medications have failed and carries the black box warning as it is considered a new class of drugs and there could be more deaths attributed to it’s use. This type of TB is rare in the US but growing in other countries and TB is spread through the air. BD
drug is pretty hefty with warnings as well and is to be used after other medications have failed and carries the black box warning as it is considered a new class of drugs and there could be more deaths attributed to it’s use. This type of TB is rare in the US but growing in other countries and TB is spread through the air. BD  more of these types of charges are appearing on medical bills, especially ones set up for outpatient services. Sometimes insurers do not pay the fees and thus some patients begin looking for doctors who do not have this charge. Facility fees are amounting up to a billion dollars a year that Medicare pays, so you wonder what is accomplished here as practices can charge more that are owned by hospitals too so does Medicare get the double whammy when they are trying to save money?
more of these types of charges are appearing on medical bills, especially ones set up for outpatient services. Sometimes insurers do not pay the fees and thus some patients begin looking for doctors who do not have this charge. Facility fees are amounting up to a billion dollars a year that Medicare pays, so you wonder what is accomplished here as practices can charge more that are owned by hospitals too so does Medicare get the double whammy when they are trying to save money?  This was a very “touch” interview of sorts. He makes good points as far as having “public” systems available with technology. Very carefully the word “nudge” is used which I think is the right terminology. He’s right with the new tools we have coming out but I don’t think the title here for this interview was maybe correct? I do not believe he is saying that the future of medicine is technology and not the doctors, again my opinion here. I would say more so he’s telling all to “pay attention” to some of the tools that are out there, and there are some good ones. Granted we get los in the “app for everything” concept that seems to breed today and finding the “value” in what we do see as being something we can use is a task. There’s crap out there too, but again I think he’s suggesting to look for the tools out there than can guide and educate.
This was a very “touch” interview of sorts. He makes good points as far as having “public” systems available with technology. Very carefully the word “nudge” is used which I think is the right terminology. He’s right with the new tools we have coming out but I don’t think the title here for this interview was maybe correct? I do not believe he is saying that the future of medicine is technology and not the doctors, again my opinion here. I would say more so he’s telling all to “pay attention” to some of the tools that are out there, and there are some good ones. Granted we get los in the “app for everything” concept that seems to breed today and finding the “value” in what we do see as being something we can use is a task. There’s crap out there too, but again I think he’s suggesting to look for the tools out there than can guide and educate.  valves should not take the drug as it was not studied in that population yet. Bristol-Meyers Squibb is the manufacturer and it will be co-marketed with Pfizer. They are a little late to the game as Pradaxa was approved about 2 years ago as an alternative for Warfarin. There are no regular blood tests required to monitor as there is with Warfarin. Eliquis could prove to be better drug however since it is in a newer class of drugs. In addition there is Xarelto that also competes in this arena. In the clinical trial of 18,000 patients those taking Eliquis had fewer strokes. BD
valves should not take the drug as it was not studied in that population yet. Bristol-Meyers Squibb is the manufacturer and it will be co-marketed with Pfizer. They are a little late to the game as Pradaxa was approved about 2 years ago as an alternative for Warfarin. There are no regular blood tests required to monitor as there is with Warfarin. Eliquis could prove to be better drug however since it is in a newer class of drugs. In addition there is Xarelto that also competes in this arena. In the clinical trial of 18,000 patients those taking Eliquis had fewer strokes. BD  law so the normal fix would be to update the IT infrastructure to either amend or send updates to policy holders and the state sounds like they saw an area of algorithm neglect here. The retirees at Nordstrom were sold 100 dental policies that had not been approved and in another area the company continued to sell a health policy that had been disapproved.
law so the normal fix would be to update the IT infrastructure to either amend or send updates to policy holders and the state sounds like they saw an area of algorithm neglect here. The retirees at Nordstrom were sold 100 dental policies that had not been approved and in another area the company continued to sell a health policy that had been disapproved. 
 and also in Orange County. You can read the article below to see where the talks failed with Tenet wanting higher rates and Health Net had their own ideas of rate increases being tied to the consumer price index. Medi-Cal was also in the picture with questions related to federal and state funding. This is effective now and the actual date was December 21, 2012 so patients and doctors will have to scramble to go elsewhere for services.
and also in Orange County. You can read the article below to see where the talks failed with Tenet wanting higher rates and Health Net had their own ideas of rate increases being tied to the consumer price index. Medi-Cal was also in the picture with questions related to federal and state funding. This is effective now and the actual date was December 21, 2012 so patients and doctors will have to scramble to go elsewhere for services.  California hospitals run by Tenet Healthcare after contract negotiations broke down.
California hospitals run by Tenet Healthcare after contract negotiations broke down. directly for hospitals and some have “goals” they somewhat enforce as the pinch for money and profits grows. Doctors normally get paid a salary from a hospital with a bonus tied in somewhere, the old pay for performance routine that insurers sell shareholders on as far as promising productivity. Doctors’ sometimes get their salaries reduced too if they don’t meet goals.
directly for hospitals and some have “goals” they somewhat enforce as the pinch for money and profits grows. Doctors normally get paid a salary from a hospital with a bonus tied in somewhere, the old pay for performance routine that insurers sell shareholders on as far as promising productivity. Doctors’ sometimes get their salaries reduced too if they don’t meet goals.  Hamburg also made similar statements in her address (video at the link below) this year to the graduating class of Einstein Medical. When you start seeing such messages over and over it appears to be a sign of the time of how difficult it is these days as a doctor to keep everyone happy on both sides.
Hamburg also made similar statements in her address (video at the link below) this year to the graduating class of Einstein Medical. When you start seeing such messages over and over it appears to be a sign of the time of how difficult it is these days as a doctor to keep everyone happy on both sides.  (NASDAQ: CPHD) today announced that it has received clearance from the U.S. Food & Drug Administration (FDA) to market Xpert® CT/NG. Running on Cepheid's GeneXpert® Systems, Xpert CT/NG is a qualitative in vitro molecular diagnostic test for the detection and differentiation of Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG). For the first time, same-day patient consultation and treatment is possible for the two most common sexually transmitted bacterial infections in the United States.
(NASDAQ: CPHD) today announced that it has received clearance from the U.S. Food & Drug Administration (FDA) to market Xpert® CT/NG. Running on Cepheid's GeneXpert® Systems, Xpert CT/NG is a qualitative in vitro molecular diagnostic test for the detection and differentiation of Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG). For the first time, same-day patient consultation and treatment is possible for the two most common sexually transmitted bacterial infections in the United States.  line had to come up with a name so those folks who understand queries and big data systems could be given a name. The term Data Scientist is not to be confused with Computer Science as we are talking two very different and distinct classifications of work. I’m not talking about “real” scientific research either as that speaks for itself. What I am talking about is “science to make money” or to find a way to make money. Sometimes as we read about some of the “monetary” incentives make their way over to the research side and some come out as frauds.
line had to come up with a name so those folks who understand queries and big data systems could be given a name. The term Data Scientist is not to be confused with Computer Science as we are talking two very different and distinct classifications of work. I’m not talking about “real” scientific research either as that speaks for itself. What I am talking about is “science to make money” or to find a way to make money. Sometimes as we read about some of the “monetary” incentives make their way over to the research side and some come out as frauds.  climb the mountain, because it’s there. Is that the case with business and some aspects of big data? Nobody knew what a quant was until they hired a few mathematicians to create non linear formulas, then of course they were the design masters of business plans as a formula could help create the framework. As time moved forward with models, they of course became a lot more than framework people, they were assigned tasks like “risk assessment” to work on to see if adjusting numbers there would lead to greater profitability and guess what, it worked well for the banks and still does.
climb the mountain, because it’s there. Is that the case with business and some aspects of big data? Nobody knew what a quant was until they hired a few mathematicians to create non linear formulas, then of course they were the design masters of business plans as a formula could help create the framework. As time moved forward with models, they of course became a lot more than framework people, they were assigned tasks like “risk assessment” to work on to see if adjusting numbers there would lead to greater profitability and guess what, it worked well for the banks and still does.  find out they have been fed a bunch of hog wash, reports and statistics to afford making money only. The link below has a video which I thought was very good as IT folks from big companies are sitting around discussing this exact topic and the one gal from T-Mobile had guts enough to say “what we are doing now is silly”..meaning she looked at what T-Mobile was doing in house, and she knew the difference between linear and non linear data sets as well as the time it takes to prepare the sets for queries, etc. She was not a data scientist either but was kind admitting she would like to find one:)
find out they have been fed a bunch of hog wash, reports and statistics to afford making money only. The link below has a video which I thought was very good as IT folks from big companies are sitting around discussing this exact topic and the one gal from T-Mobile had guts enough to say “what we are doing now is silly”..meaning she looked at what T-Mobile was doing in house, and she knew the difference between linear and non linear data sets as well as the time it takes to prepare the sets for queries, etc. She was not a data scientist either but was kind admitting she would like to find one:) and can imagine how it might grow to stifle itself as the OMG media and drama queen stories pick up with the “good guy” “bad guy” routines with driving emotions. We find this today amass in the media instead of an alternative of some helpful logic. “Data Scientists” as they exist and continue to grow will be anything but drama with their research and again is this science, really? BD
and can imagine how it might grow to stifle itself as the OMG media and drama queen stories pick up with the “good guy” “bad guy” routines with driving emotions. We find this today amass in the media instead of an alternative of some helpful logic. “Data Scientists” as they exist and continue to grow will be anything but drama with their research and again is this science, really? BD  will be asking the same question. This is not to be confused with “insurance exchanges” in this instance as this is for sharing medical records only. The group has gone to insurance companies to see if they will kick in some money. I wouldn’t be one to hold my breath on that one but you never know, but grants seem to be more the way to get funded with medical health data if they can be had.
will be asking the same question. This is not to be confused with “insurance exchanges” in this instance as this is for sharing medical records only. The group has gone to insurance companies to see if they will kick in some money. I wouldn’t be one to hold my breath on that one but you never know, but grants seem to be more the way to get funded with medical health data if they can be had. 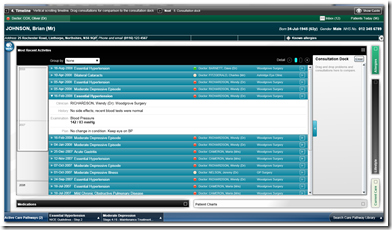

 This is a photo sent to Reportit by FOX10 News viewer Michael Whitehead. He said this is second floor of Mobile Infirmary after a tornado struck Mobile on December 25.
This is a photo sent to Reportit by FOX10 News viewer Michael Whitehead. He said this is second floor of Mobile Infirmary after a tornado struck Mobile on December 25. 

 supporter who has committed $100 million to St. John's and has his name on several buildings was shocked when the CEO and board recently were fired by the current Catholic out of state owners as it was in the works to sell the hospital. Soon-Shiong said he would like to see the hospital back in the hands of local owners and he was also ready to help finance the sale. St. John's is the only California hospital run by the Sisters of Charity in Denver. The hospital was opened after World War 2 and has taken care of many celebrities in it’s time and has it’s Hollywood connections with philanthropy as well. When Santa Monica Bay Physicians joined the UCLA Health System in 2010 St. Johns lost a bit of business.
supporter who has committed $100 million to St. John's and has his name on several buildings was shocked when the CEO and board recently were fired by the current Catholic out of state owners as it was in the works to sell the hospital. Soon-Shiong said he would like to see the hospital back in the hands of local owners and he was also ready to help finance the sale. St. John's is the only California hospital run by the Sisters of Charity in Denver. The hospital was opened after World War 2 and has taken care of many celebrities in it’s time and has it’s Hollywood connections with philanthropy as well. When Santa Monica Bay Physicians joined the UCLA Health System in 2010 St. Johns lost a bit of business.  turned down back in 2010 as the FDA was concerned about the side effects, bronchial spasms. This is interesting when you read this article as they were just about out of money if I an reading this correctly and were trying to find a buyer.
turned down back in 2010 as the FDA was concerned about the side effects, bronchial spasms. This is interesting when you read this article as they were just about out of money if I an reading this correctly and were trying to find a buyer.  providing speed of therapeutic onset that is comparable to intravenous (IV) administration but with greater ease, patient comfort and convenience.
providing speed of therapeutic onset that is comparable to intravenous (IV) administration but with greater ease, patient comfort and convenience.  journal for a new generation of both doctors AND patients. Leveraging the power of an online, crowd-sourced community platform, Curēus promotes medical research by offering tools that better serve and highlight the people who create it, resulting in better research, faster publication and easier access for everyone.
journal for a new generation of both doctors AND patients. Leveraging the power of an online, crowd-sourced community platform, Curēus promotes medical research by offering tools that better serve and highlight the people who create it, resulting in better research, faster publication and easier access for everyone.  number of open-access journals including
number of open-access journals including  taking statins to reduce cholesterol. Tredaptive, the drug from Merck was a combination extended release of Niacin with laropiprant that reduces facial flushing in patients as that is a side effect of Niacin. Tredaptive is approved in other countries but did not make FDA approval in the US, so it looks like the FDA was on target here. Now Niaspan, made by Abbott will probably be questioned as well as the NIH found that it offers no benefit over just using statin drugs alone. BD
taking statins to reduce cholesterol. Tredaptive, the drug from Merck was a combination extended release of Niacin with laropiprant that reduces facial flushing in patients as that is a side effect of Niacin. Tredaptive is approved in other countries but did not make FDA approval in the US, so it looks like the FDA was on target here. Now Niaspan, made by Abbott will probably be questioned as well as the NIH found that it offers no benefit over just using statin drugs alone. BD  words is it breast cancer or kidney cancer that migrated to the lungs. The targets to treat are very specific and thus we have read stories of patients being given the wrong medication with treating “lung” cancer that originated in the kidney, so thus it is really kidney cancer and not lung cancer. There have been attempts in the past to do this but they have not worked.
words is it breast cancer or kidney cancer that migrated to the lungs. The targets to treat are very specific and thus we have read stories of patients being given the wrong medication with treating “lung” cancer that originated in the kidney, so thus it is really kidney cancer and not lung cancer. There have been attempts in the past to do this but they have not worked.  I can’t think of any and some stated that portions of what it taught is no longer applicable so some of that can be discontinued. Just in the last 5 years being a doctor has changed so much with technology and when you think back to someone who graduated even 10 years ago, we had nowhere what we have today.
I can’t think of any and some stated that portions of what it taught is no longer applicable so some of that can be discontinued. Just in the last 5 years being a doctor has changed so much with technology and when you think back to someone who graduated even 10 years ago, we had nowhere what we have today.  by leaps and bounds so does the intelligence on what they determine you are going to be shown as a price for a product. The store as an example here for most of this article is Staples. So much for everyone being offered the same price for the same product anymore:) We all hear that the financial world uses mathematics that are way too complicated, said by the quants themselves. Well here we go with trying to buy a simple stapler according to the Wall Street Journal and their recordings of the event.
by leaps and bounds so does the intelligence on what they determine you are going to be shown as a price for a product. The store as an example here for most of this article is Staples. So much for everyone being offered the same price for the same product anymore:) We all hear that the financial world uses mathematics that are way too complicated, said by the quants themselves. Well here we go with trying to buy a simple stapler according to the Wall Street Journal and their recordings of the event.  sense on some of this real time adjusting pricing in the fact that if it picks up tremendously, that sites can in fact experience the same thing as we see in markets today with flash crashes as now you have a ton more algorithms at work to keep that data changing all the time, it is what it is so retailers look like they are taking some lessons from the financial markets, and is all of this data activity really necessary to promote more profitability and how much is it really generating is the question. The more code you run and change things, the greater your chances are for some rogue algorithms to kick in and potentially mess everything up. When I say rogue let’s say you were given the lower price but at the time of check out did something go wrong and charge you the higher price? Expect things like this to occur as it happens all the time with shifting and changing data at rapid speeds and rates. A few errors like the potential example above might be enough to cut out some complex algorithms that really do not need to be there.
sense on some of this real time adjusting pricing in the fact that if it picks up tremendously, that sites can in fact experience the same thing as we see in markets today with flash crashes as now you have a ton more algorithms at work to keep that data changing all the time, it is what it is so retailers look like they are taking some lessons from the financial markets, and is all of this data activity really necessary to promote more profitability and how much is it really generating is the question. The more code you run and change things, the greater your chances are for some rogue algorithms to kick in and potentially mess everything up. When I say rogue let’s say you were given the lower price but at the time of check out did something go wrong and charge you the higher price? Expect things like this to occur as it happens all the time with shifting and changing data at rapid speeds and rates. A few errors like the potential example above might be enough to cut out some complex algorithms that really do not need to be there.