

The comment below from a vendor is interesting, as he comments on the fact that a physician can make an extra $125,000 in 5 years, well some family care practice doctors today in California would like to just be making that in one year, as all the recent contracts with insurance companies are getting more stringent and mal practice certainly is not going down, salary is what is left after the bills are paid.
“But physicians also need to understand that this is an investment, so they will not only make their initial costs back, but in the next five years, they could make an extra $125,000.”
The problem with many EHR systems is that they were designed by software engineers who may not be familiar with how doctors work, adds Thornton.
That is valid as there are two head that need to come together here, the programmer and the phy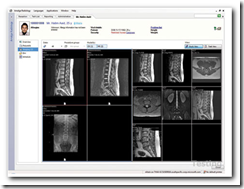 sician for a useable piece of software, been there and done that from the programmer side and worked with an MD.
sician for a useable piece of software, been there and done that from the programmer side and worked with an MD.
You can also read here from a blogging Physician, Kevin, MD as featured in USA today.
Bottom line on most of this though is the money as everyone else benefits more than the physician so hospitals need to subsidize. If you have been reading the blog, I have posted 3 stories in the last week of hospitals doing just this, as the EHRs need to communicate with the hospitals where they are on staff.
An integrated system by far is needed and there are systems that run off a remote server and can provide a local back up of records for the physician too, problem solved there with a properly designed architecture.
As for the user experience I am a software person, and this stuff is beginning to make me crazy, and I love software! If a physician is on staff at more than one hospital, there might be more than one system to learn, so is that enough to make you crazy, I think so, thus I think the move towards one common user interface is going to get pretty popular very soon. Here’s a video I did a short while back, just me poking around the interface.

I have written about this before with the Common User Interface from Microsoft, open source, Silverlight technology, available for download on Code Plex, the Microsoft Open source site.
You can run your individual services at the back end on the server and work towards the same or very similar interface at the front end, just write the code and there’s open source Linux called “Moonlight” to help out there too. There’s a lot of code already developed, so why re-invent the wheel at this point and worry about who might have the “better” code, let’s all build off of one format, at least at the front end for the users. Visit a Microsoft Tech center
Ask any doctor if they would like to see the same interface where ever they go and I can almost bet you would not hear one complaint if that were to happen as it would stand to make their lives as healthcare clinicians much simpler. The interest for a common interface is in fact starting to grow.
A simplified system along with the same interface would really help accelerate the problem of adaptation and subsidies from the hospitals will help make this happen.
 Now what if the hospital doesn’t have the money, and is perhaps one of the “Desperate Hospitals” I have covered in my series on insolvent hospitals? Get those fundraisers and charity events and websites up and going.
Now what if the hospital doesn’t have the money, and is perhaps one of the “Desperate Hospitals” I have covered in my series on insolvent hospitals? Get those fundraisers and charity events and websites up and going.
Actually I would like to see CMS dedicate a site to help drive contributions to those hospitals who need help and see CMS do something charitable, certainly couldn’t hurt.
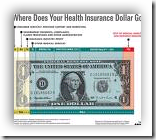
First on the list for charity contributions, insurance companies who have huge amounts of “reserves” for the “just in case” scenarios and this could very well fit the bill there. In California, insurance companies spent more than 10 billion last year on profits and administration.
The 3 major insurance carriers in the state of Washington recently reported a cash surplus of $2.2 Billion (with a B) for the year 2006...any guess on what the cash reserves for the State of California might be and this information is almost 2 years old and you can bet the surpluses are growing, thus I think donations to help keep our hospitals in business could very well be afforded and in good faith from the insurance carriers as they seem to find funds or all types of other projects including paying patients to take their medications.
EHRs go under too if they don’t get paid. BD
To many, it’s no big surprise that electronic health record (EHR) systems have had a slow adoption rate. Besides the cost and learning curve involved, physicians have seen several EHR companies go under, and that’s made them even more apprehensive about investing in the technology.
But a recent New England Journal of Medicine study sheds some light on just how slow those rates have been. According to the study, only 4% of U.S. physicians use comprehensive EHR systems, including safety features such as drug interaction prompts. Another 13% say they use a more basic EHR system without the added safety features.
http://www.fortherecordmag.com/archives/ftr_091508p12.shtml
Hi Barbara!
ReplyDeleteThe last 2 paragraphs about EHR slow adoption rates and why it's so is important... can't be said enough times.
Al
Thanks Al for stopping by, yes we need a simpler solution as there are so many programs and it's getting to be a complicated situation for the physicians all over, if there were a common user interface someday, that could certainly help the numbers of folks that adopt.
ReplyDelete