 Two probable swine flu cases found in Irvine, CA- Update
Two probable swine flu cases found in Irvine, CA- Update
The test results should be in soon to confirm. Neither individual knew the other one and both had recently been to Mexico, so it appears t...


Four Preview Videos in the Footer
Two probable swine flu cases found in Irvine, CA- Update
The test results should be in soon to confirm. Neither individual knew the other one and both had recently been to Mexico, so it appears t...
 Hospital MRI and Other Medical Devices Infected with Conficker Virus – FDA Required 90 Day Notice before Windows Update Patch Could be Applied
Hospital MRI and Other Medical Devices Infected with Conficker Virus – FDA Required 90 Day Notice before Windows Update Patch Could be Applied
This is an interesting story all the way around. First of all I hope all the medical devices found were disconnected from the Internet unti...
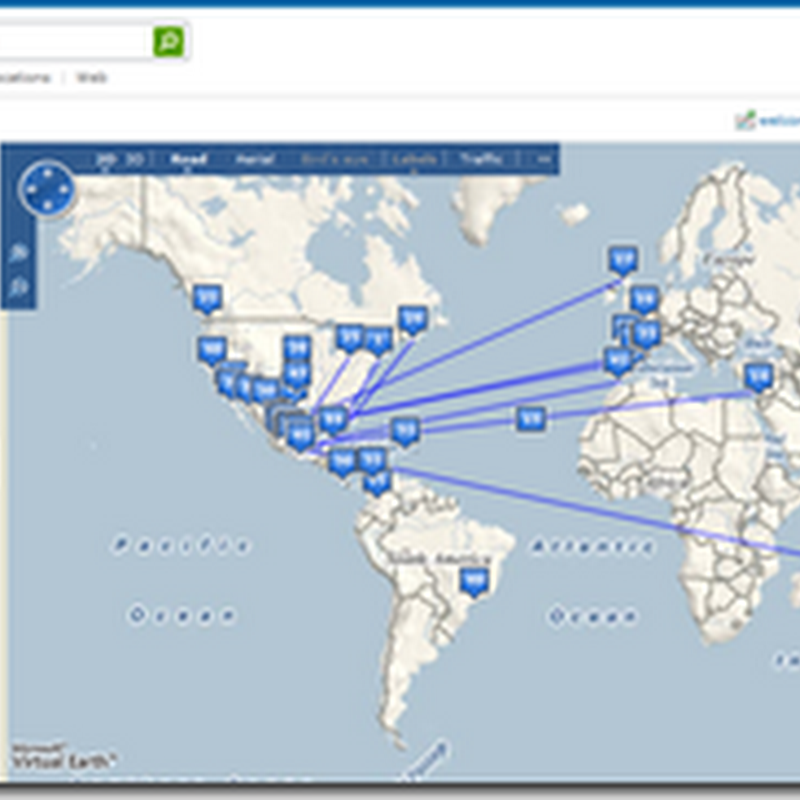 Amalga at El Camino Hospital Helping to Monitor the Status of Swine Flu – everyone can use Virtual Earth for Global Tracking
Amalga at El Camino Hospital Helping to Monitor the Status of Swine Flu – everyone can use Virtual Earth for Global Tracking
Yesterday I posted about Microsoft Amalga and the New Life Sciences software to be added. I mention this as the Life Sciences folks are the...
 Swine flu Moving Closer to Orange County, CA – One probable case at Cal State Long Beach
Swine flu Moving Closer to Orange County, CA – One probable case at Cal State Long Beach
This is California, the Long Beach campus gave out masks and flooded with news, but few were wearing them, unlike what we saw in the CNN vid...
 Chief Complaint Swine Flu -Video from Mexico
Chief Complaint Swine Flu -Video from Mexico
CNN put out a video showing what it looks like in Mexico, including a hospital and how healthcare professionals are reacting and treating pa...
 Security tightened over data loss – Flash Drives Can be One of HealthCare’s Biggest Nightmares
Security tightened over data loss – Flash Drives Can be One of HealthCare’s Biggest Nightmares
This even happened in the UK, but it can happen anywhere. I have seen it here, flash drives lost containing patient information, and somet...
 Microsoft's Tellme Voice Service For Windows Mobile Cell Phones Coming Soon
Microsoft's Tellme Voice Service For Windows Mobile Cell Phones Coming Soon
This is great news for the new operating system for Windows Mobile. I use a Windows Mobile Cell Phone and already use some of the voice co...
 Making Money from the Swine Flu – Shirts and Games Appear on the Web
Making Money from the Swine Flu – Shirts and Games Appear on the Web
With the way advertising works today and the internet, it didn’t take long for shirts and games to appear. If you don’t get enough with ju...
 California Outpatient Centers Offering 23andMe Genome Service
California Outpatient Centers Offering 23andMe Genome Service
This shows a clear new effort to help educate patients on what their genetic background could hold in store, and is one more step with brin...
First Death Victim of Swine Flu in US was visiting from Mexico
The State of Texas is especially on alert with those crossing over the border. BD HOUSTON — A 23-month-old boy from Mexico City becam...
 Dr. Sanjay Gupta in Mexico – Masks are Everywhere
Dr. Sanjay Gupta in Mexico – Masks are Everywhere
This is also very interesting what he has to say about the strain, and what makes up the composition. It is called the Swine flu as that co...
 Dendreon Day - What Got People More Excited, the Announcement or the Stock?
Dendreon Day - What Got People More Excited, the Announcement or the Stock?
A current treatment, docetaxel (Taxotere) has some pretty bad side effects, but Provenge can extend life without the nasty chemo effects. ...
 Global Map to View Swine Flu Alerts – HealthMap for Global Disease
Global Map to View Swine Flu Alerts – HealthMap for Global Disease
The site will give a quick visual on where Swine Flu is and has been reported. This is what it looks like today and lucky folks in Alaska a...
 What’s a Drug Rep’s Worst Enemy – A Computer, Maybe?
What’s a Drug Rep’s Worst Enemy – A Computer, Maybe?
According to this study, the virtual reps with the e-promotions are turning out to be a bit more popular. Just like anything else that is ...
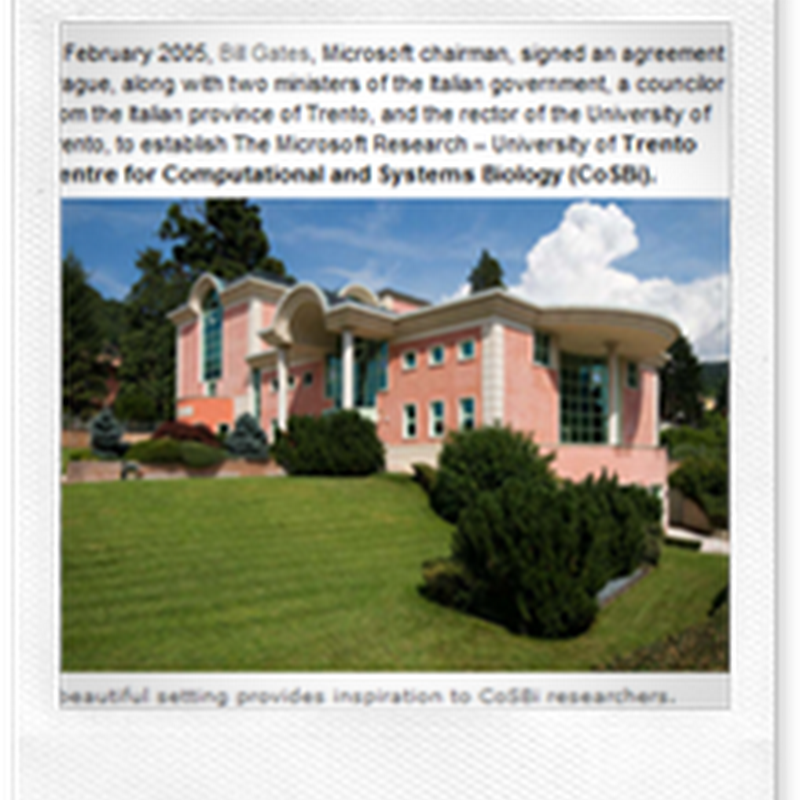 Microsoft Introduces Groundbreaking Technology – Amalga Life Sciences Software
Microsoft Introduces Groundbreaking Technology – Amalga Life Sciences Software
There’s quite a bit going on this week, and one expo in particular is the Annual Bio-IT Conference. Today, Microsoft announced Amalga Lif...
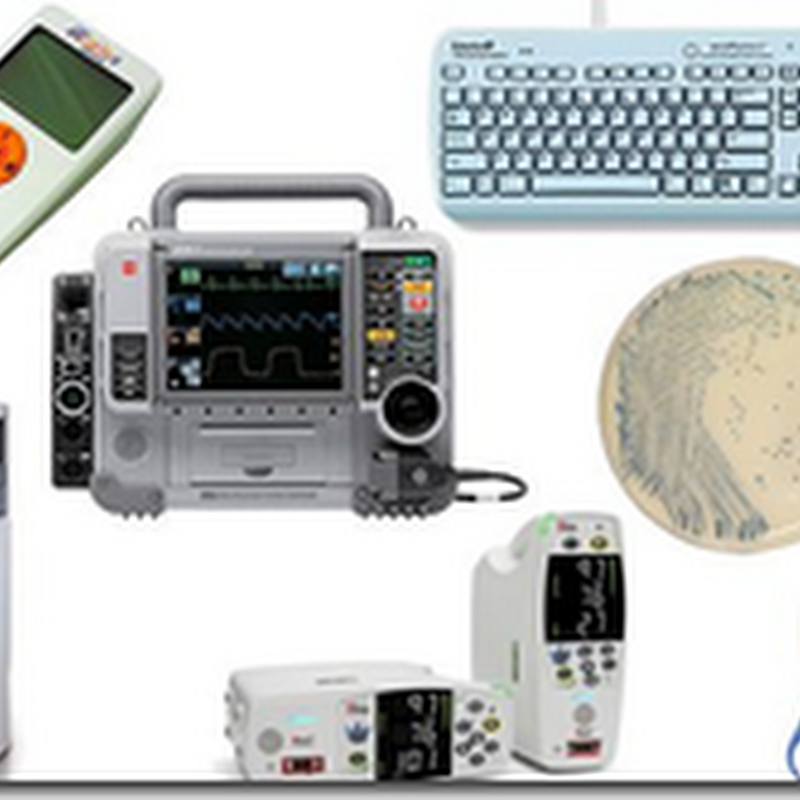 BusinessWeek – Medical Device Award Winners
BusinessWeek – Medical Device Award Winners
One product mentioned in the winner’s circle is Merlin. You can do a search of the blog as I have several posts relative to the product fr...
 Tweeting for Trials – TrialX Wins New York Entrepreneur Week Venture Competition Award
Tweeting for Trials – TrialX Wins New York Entrepreneur Week Venture Competition Award
I have been somewhat following this company since they started out, and at that point were questioning if there was in fact a market for thi...
 Belly dancers Rally for Better Health Care in Seattle
Belly dancers Rally for Better Health Care in Seattle
They have to usually find their own private insurance plans, hope the weather was nice that day. BD Small rallies in favor of a nati...
 Influenza Tracking Project – Now You Can Talk about it on Facebook
Influenza Tracking Project – Now You Can Talk about it on Facebook
If you have the flu, Swine or otherwise and want to talk about it to help researchers, here’s the place on Facebook. Information will be t...
Johns Hopkins Health System Acquires Suburban Hospital – Bethesda, MD
The Suburban Hospital location is right across the street from the NIH, so this is probably a very good strategic move with the relations t...
 Regulators again criticize conditions at Anaheim General Hospital – Orange County, CA
Regulators again criticize conditions at Anaheim General Hospital – Orange County, CA
A few more blows for this hospital trying to survive. It has already lost it’ accreditation from the Joint Commission. Not a good idea pe...