

AAFP wants to be able to include family care physicians. I think if this gets any more confusing you can toss it out and start over as it’s so complicated. Granted there is some good work being done in different areas and it all depends on Health IT to successfully implement an ACO. On top of that you have insurers wanting to come in and kind of guide the ACO too, so who does run the show? The rules of the ACO were vague as rules go and each ACO is it’s own story book you could say.
With all the data and areas of concern to be examined, 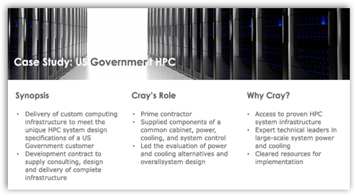 modeled and predicted, better get some kick ass computer power like this new Cray unit coming out and let’s do some of this like Wall Street and Fortune 500 companies do with analyzing big chunks of data and running some SQL queries to sort all of this out, otherwise with everything moving so fast today, we don’t have time and the ones who have the data capabilities have the money and will keep it and create additional algorithms to get more. It is what it is and some government offices are already using it. The video below talks about improvements one organization made, and this is Johns Hopkins and Miami talking so where does this leave everyone else. Get a Cray and get the data for a better starting point.
modeled and predicted, better get some kick ass computer power like this new Cray unit coming out and let’s do some of this like Wall Street and Fortune 500 companies do with analyzing big chunks of data and running some SQL queries to sort all of this out, otherwise with everything moving so fast today, we don’t have time and the ones who have the data capabilities have the money and will keep it and create additional algorithms to get more. It is what it is and some government offices are already using it. The video below talks about improvements one organization made, and this is Johns Hopkins and Miami talking so where does this leave everyone else. Get a Cray and get the data for a better starting point.
Cray Introduces 50-Petaflop XK6 Supercomputer–First Client is the Swiss National Supercomputing Centre For Medical Research–An Upgrade in Computing Power
We had GOP Senators today wanting a re-write too, so this is non partisan with issues and complaints. If things get too hard and you can’t see light at the end of the hallway, people give up and in come the insurers with their algorithms and then everyone wonders why this keeps happening. We can’t keep taking dull knives to gun battles and at least get some information up front that is factual and do some high powered simulations.
Everyone thinks pilots do such a good job with simulation so why can’t we simulate an ACO, drugs are being made this way too with simulating on computers and only the very last stage is a wet lab even created.
Actually it’s kind of funny as I have had a couple pilots write and said they wished that everyone would quit comparing healthcare to being pilot as pilots are not doctors and doctors are not pilots, unless you have the one who faked out the AMA, but he lost in the end. He is a real pilot but a fake doctor:)
Pilot At United Airlines Claimed to be an MD and Duped Many, Including the AMA With Phony MD Credentials
I am not saying the computer is going to kick out a magic answer as that still comes from interpretations, but do you think your chances are better at making a touch down when you are at the 10 yard line versus the 40 yard line?
In other words use the computer to move forward to eliminate as much as the unintended circumstances as possible and look at real numbers, data and information. I like living here in the US and want a “smart” legislative process with digital literate lawmakers who can compete and work on the same levels as Fortune 500 companies and Wall Street and if you watch the news, it’s not happening and the farther behind we fall. Below are 2 bills that wasted time as the IT Infrastructure they suggest can’t be met, again digital literacy needed soon, please! BD
Two More Senators Propose More Bills to Publish Medicare Claims Data Without A Hint of Digital Literacy Relative to Cost and Time
Although properly structured accountable care organizations, or ACOs, can make America's health care delivery system "more accountable and more focused on value instead of volume," the AAFP is concerned that, as currently proposed, Medicare's ACO program "will fail to offer the potential benefits of better care for individuals, better health for populations, lower per capita costs for Medicare beneficiaries and improved coordination among physicians." That was the message AAFP Board Chair Lori Heim, M.D., of Vass, N.C., recently sent to CMS Administrator Donald Berwick, M.D.
In particular, the AAFP urged CMS to
- create alternative policies to allow primary care physicians to participate in multiple Medicare ACOs;
- employ a variety of payment approaches, such as blended fee-for-service payments and episode/case rate payments;
- outline quality reporting requirements for the full three-year program and reduce the number of required quality measures;
- offer greater program flexibility to encourage small and medium-sized primary care practice participation; and
- ensure that primary care physicians hold top leadership positions in ACOs.
The AAFP also asked Berwick to retain only those measures that improve population health outcomes and efficiency.
The best way to modify physician behavior -- a considerable challenge for any ACO -- is to pay physicians in a timely manner for their services, whether those services are provided directly in a physician's practice or via e-mail or telephone consultation, said Heim.
According to Heim, the Academy also has concerns about the proposed quality measure scoring process, the overall performance score, the performance benchmarks and the minimum attainment level for each quality measure. "These types of complexities further exclude smaller and less-integrated primary care practices," she said.
0 comments :
Post a Comment